article reprinted from the McPherson Eye Research Institute’s Fall 2024 InSights newsletter
Dr. Roomasa Channa is a retina surgeon with a research focus on preventing vision loss from diabetes. Throughout her career, her clinical work has been the inspiration for her research. As a trainee, one of her first patients on call was a young African-American woman from inner city Baltimore. She presented to the emergency room with sudden vision loss and headaches, thinking she was having a migraine. Dr. Channa noted that one of the patient’s eyes was full of blood, and the other had the classical findings of advanced diabetic retinal disease. The patient was unaware that she even had diabetes and severely uncontrolled blood sugars.

Diabetes is the leading cause of vision loss among working aged adults in the U.S., but Dr. Channa has long thought that advanced diabetic eye disease is preventable with screening and early detection. However, as the number of patients with diabetes increases, it has become burdensome to both patients and providers to perform the annual eye screenings recommended by the American Diabetes Association and the American Academy of Ophthalmology. This burden is disproportionately higher for patients from socioeconomically disadvantaged backgrounds due to inequities in our health system. Solving the problem of poor access to eye care became Dr. Channa’s driving research interest and coincided with growing interest in ophthalmology to use artificial intelligence to address this problem.
Diabetic retinal diseases have very characteristic findings on retinal images (pictures your eye doctor routinely takes to document how your retina looks), findings that were established at the Wisconsin Reading Center. These readily identifiable indicators make it possible to train a computer to do the repetitive task of searching these images for characteristic abnormalities. Currently, we have multiple AI programs that can automatically detect diabetic retinopathy from retinal images. Dr. Channa’s lab analyzes the ability of these AI approaches to prevent vision loss from diabetes, which is needed to maximize their effectiveness in the clinic.
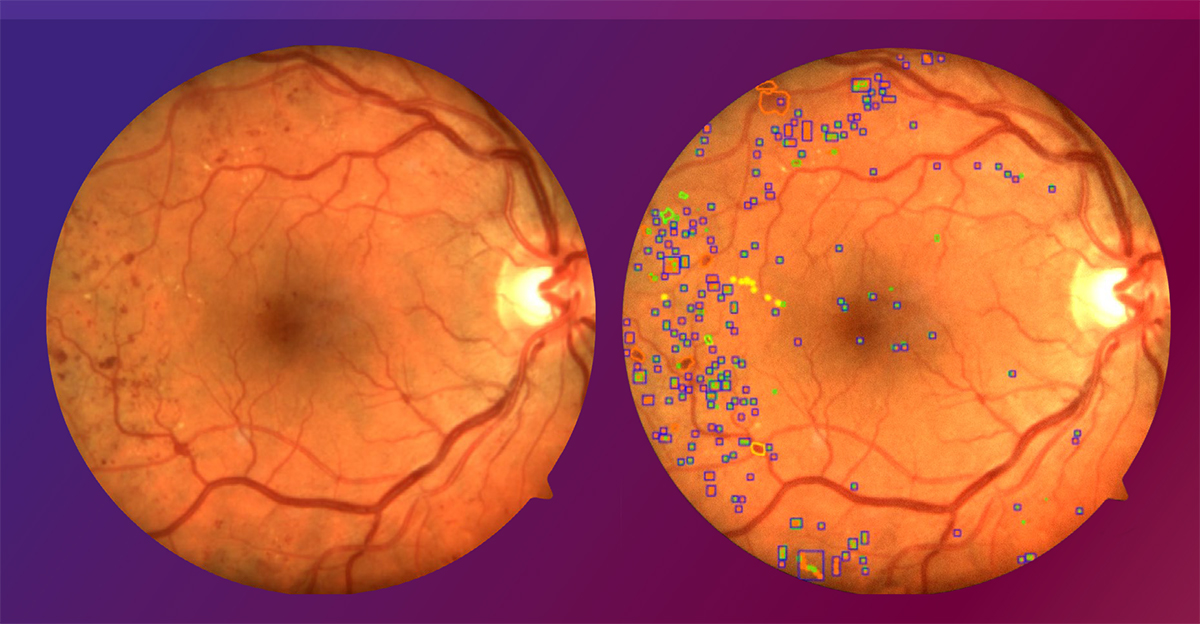
A retinal scan of a patient with diabetic retinopathy. In the image on the right (and on the cover of this issue), diabetic retinopathy lesions are outlined by an AI algorithm. Image courtesy of Roomasa Channa, MD.
The model developed in Dr. Channa’s lab is called the Care Process for Preventing Vision Loss from Diabetes (CAREVL) model, and it has already determined that AI-based eye screening (as opposed to traditional in-person screening at an eye doctor’s office) could prevent severe vision loss in an additional 27,000 patients with diabetes across the U.S. The effect could be further increased 3-to-4-fold by optimizing “next steps” in the care process, such as following up with recommended eye treatments. Based on this and previous work, the Channa Lab designed a screening strategy termed AI-BRIDGE (Artificial Intelligence-Based point of caRe, Incorporating Diagnosis, schedulinG, and Education) to address the problem of poor adherence with screening and eye care follow-up.
The AI-BRIDGE strategy begins with eye imaging and identification of eye disease in primary care clinics using AI-based analysis. It then facilitates follow-up by providing patients with culturally-adapted education regarding diabetic eye disease, and then helping local clinics schedule eye appointments. An upcoming multi-center clinical trial, funded by a 5-year, $4.7 million R01 grant from NIH/NEI, will test whether the AI-BRIDGE screening strategy improves diabetic eye care access across different racial and ethnic groups compared to standard approaches.
The implementation of AI-based eye screening in underserved settings has been challenging, and there is the risk that pervasive eye care disparities will be worsened if AI-based screening is adopted by only large academic centers, and ignored in other settings. Dr. Channa’s upcoming multi-center trial will include underserved primary care clinics and work to seamlessly integrate this technology into their busy workflows. Ultimately, the trial will assess whether AI screening technology can decrease racial, ethnic, and socioeconomic disparities in vision loss.
Dr. Channa’s lab also employs AI to study how retinal damage first begins in diabetes, with the goal of halting it as soon as possible. For example, the initial effects of high blood sugar may not affect the blood vessels of the retina like most researchers assume; rather, it may alter the retinal cells themselves. With the help of computer scientists at UW-Madison, she is leading a prospective trial at the UW Department of Ophthalmology and Visual Sciences that uses AI to analyze retinal images with the goal of uncovering changes in diabetic retinal disease before they are visible to human examiners.
Taken together, Dr. Channa’s comprehensive, cutting-edge research provides great hope to a nation striving to address a rapidly growing burden of vision loss from diabetes in all segments of our population.